Complete vs Partial Mole: Understanding Key Differences
Complete vs Partial Mole: Understanding Key Differences
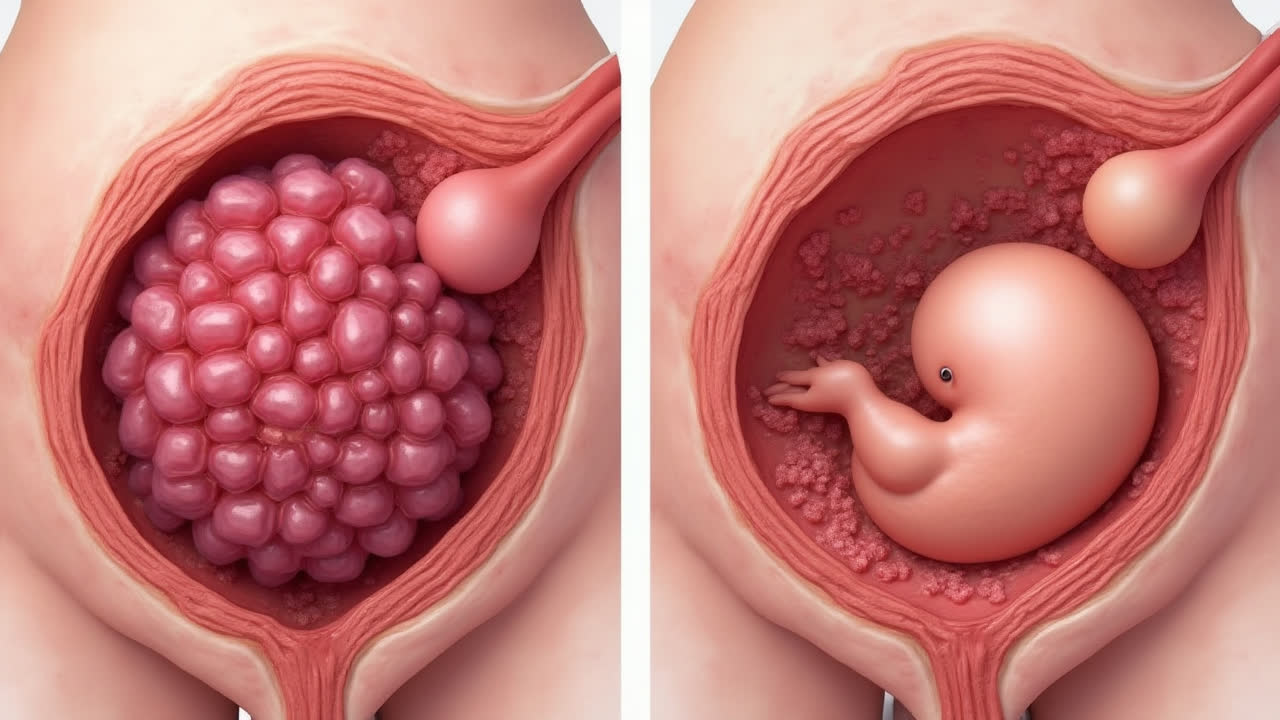
When it comes to pregnancy complications, molar pregnancies stand out as particularly complex and potentially concerning. The main difference between complete mole and partial mole lies in their chromosomal makeup and development pattern - a complete mole occurs when an empty egg (without DNA) is fertilized by one or two sperm, while a partial mole develops when a normal egg is fertilized by two sperm or one abnormal sperm.
Understanding these two types of molar pregnancy is crucial for proper diagnosis and treatment. Both are forms of gestational trophoblastic disease, where abnormal tissue grows instead of a viable pregnancy. Have you ever wondered how these rare pregnancy complications actually form and what makes them different? It's fascinating from a medical standpoint, though obviously concerning for those experiencing it.
What is a Complete Mole?
A complete hydatidiform mole forms when one or two sperm fertilize an egg that has lost its nucleus (the part containing DNA). Since the egg lacks maternal DNA, the sperm's DNA duplicates to create a diploid cell with only paternal genetic material. This is why about 90% of complete moles have a 46,XX karyotype, while 10% show 46,XY.
The absence of maternal DNA means no fetus develops in complete moles. Instead, the abnormal tissue proliferates dramatically, causing significantly elevated hCG (pregnancy hormone) levels. This often leads to rapid uterine enlargement and dramatic symptoms. I find it remarkable how the body's attempt to create new life can sometimes go so spectacularly awry.
Symptoms typically include severe vaginal bleeding, hyperemesis (extreme nausea), and in later stages, hyperthyroidism. The ultrasound appearance is quite distinctive - it's often described as a "snowstorm" pattern. It's honestly one of the most striking findings in obstetric imaging.
The risk of developing choriocarcinoma (a malignant form of trophoblastic disease) is notably higher with complete moles - about 15-20%. This means close monitoring after treatment is absolutely essential.
Understanding Partial Molar Pregnancy
A partial mole occurs quite differently. Here, a normal egg is fertilized by either two sperm or one abnormal sperm with duplicate DNA. This creates a triploid cell (69 chromosomes instead of the normal 46). Unlike complete moles, partial moles contain both maternal and paternal DNA.
The presence of maternal DNA allows for some fetal development, though the fetus is invariably non-viable. These pregnancies often present with moderately elevated hCG levels rather than the dramatically high levels seen in complete moles. The uterus may even measure smaller than expected for gestational age.
Partial moles are actually less common than complete moles and carry a lower risk of malignancy - only about 1-5% develop into invasive disease. That's reassuring news for patients dealing with this diagnosis.
Interestingly, partial moles are often initially misdiagnosed as spontaneous abortions. It's only after pathological examination of the tissue that the true diagnosis emerges. This delayed diagnosis can sometimes create anxiety for patients.
Comparison Table: Complete vs Partial Mole
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Formation | Empty egg + 1-2 sperm | Normal egg + 2 sperm (or abnormal) |
| Chromosomes | 46,XX or 46,XY (diploid) | 69,XXY or 69,XXX (triploid) |
| DNA Present | Only paternal | Both maternal and paternal |
| Fetal Tissue | None | Some (non-viable) |
| hCG Levels | Very high | Moderately elevated |
| Malignancy Risk | 15-20% | 1-5% |
| Frequency | More common | Less frequent |
| Uterine Size | Rapid enlargement | Often smaller than date |
| Diagnosis | First trimester ultrasound | Usually pathology report |
Clinical Implications and Follow-up
The management of both types of molar pregnancy typically involves surgical evacuation followed by careful monitoring of hCG levels. The duration and intensity of follow-up differ based on the type of mole and individual risk factors.
With complete moles, the follow-up is more intensive due to the higher malignancy risk. Most guidelines recommend weekly hCG monitoring until levels normalize, then monthly checks for 6-12 months. For partial moles, the monitoring period may be shorter, though it varies by institution.
Sometimes I think about how challenging it must be for patients to wait through this monitoring period, especially since they're advised to avoid pregnancy during this time. The psychological impact of these complications shouldn't be underestimated.
Preventive Measures and Risk Factors
While there's no sure way to prevent molar pregnancies, understanding risk factors can help with early detection. Advanced maternal age (over 35) and very young age (under 20) both increase risk. Previous molar pregnancy is perhaps the biggest risk factor.
Early prenatal care plays a crucial role in identifying these conditions. That initial ultrasound can sometimes catch complete moles early, though partial moles often fly under the radar initially. It makes you appreciate the importance of those routine pregnancy checkups.
Adequate folic acid intake may help reduce risks of some pregnancy complications, though its specific role in molar pregnancy prevention isn't fully established. Still, it's generally recommended for all women trying to conceive.
Emotional and Psychological Support
Dealing with a molar pregnancy diagnosis can be emotionally devastating. Many women experience grief similar to miscarriage, but with the added stress of potential malignancy. Support groups and counseling can be invaluable during this time.
It's important for patients to understand that with proper treatment and follow-up, the long-term outlook is excellent. Most women who complete treatment successfully go on to have healthy pregnancies later. Hope is important during the healing process.
Frequently Asked Questions
How common are molar pregnancies?
Molar pregnancies occur in approximately 1 in 1,000 to 1 in 1,500 pregnancies in the United States. Complete moles are more frequent than partial moles, with complete moles accounting for about 50% of all cases in North America. The incidence varies by geographic region and ethnicity.
Can I get pregnant again after a molar pregnancy?
Yes, most women can successfully have normal pregnancies after a molar pregnancy. However, doctors typically recommend waiting 6-12 months after completing treatment before trying to conceive again. This waiting period allows for proper monitoring of hCG levels to ensure the mole is completely resolved and reduces the risk of recurrence.
What are the warning signs of a molar pregnancy?
Warning signs of molar pregnancy include vaginal bleeding (occurring in about 75% of cases), unusually severe morning sickness, rapid uterine growth (the uterus feels larger than expected for the gestational age), and high blood pressure before 20 weeks. Some women may experience symptoms of hyperthyroidism due to extremely high hCG levels.